Abstract
The study published in “Zhejiang Journal of Traumatic Surgery” investigates the role of transpedicular grafting of injectable artificial bone in promoting healing of fractured vertebrae during pedicle screw reduction and internal fixation for thoracolumbar fractures. A retrospective analysis was conducted on patients with thoracolumbar fractures treated with posterior pedicle screw-rod fixation and distraction reduction. Simultaneously, transpedicular implantation of self-setting calcium phosphate artificial bone was performed in the injured vertebrae.
Postoperative follow-up ranged from 1.8 to 2.2 years. Vertebral body height restoration and Cobb angle correction were measured. Fracture healing was evaluated using computed tomography (CT), and postoperative low back pain scores were compared.
Results showed that all procedures were successfully completed. The anterior vertebral height was satisfactorily restored, and the Cobb angle was significantly corrected compared to preoperative values. The anterior vertebral height recovery rate reached 90.1%, and kyphosis correction averaged 15.2°. Follow-up demonstrated good bone healing in grafted vertebrae, with no significant loss of Cobb angle after implant removal and no secondary low back pain.
Background
Thoracolumbar fractures account for approximately 80% of all spinal fractures. In recent years, surgical management has focused not only on restoring spinal alignment and decompressing neural elements but also on optimizing surgical details to improve outcomes.
Pedicle screw placement in the fractured vertebra combined with transpedicular bone grafting facilitates restoration of vertebral height, maintains spinal stability, and effectively reduces postoperative loss of Cobb angle after distraction reduction. This study reports clinical outcomes of thoracolumbar fractures treated with pedicle screw fixation combined with transpedicular injectable artificial bone grafting at the Second Affiliated Hospital of Tianjin University of Traditional Chinese Medicine.
Methods
Study Population
A retrospective analysis was performed on 25 patients with thoracolumbar fractures treated with pedicle screw fixation combined with injectable artificial bone grafting. The cohort included 17 males and 8 females, aged 45–65 years (median 56.5 years).
All patients had thoracolumbar injury classification and severity score (TLICS) values ranging from 4 to 6. Injury mechanisms included 9 cases of traffic accidents and 16 cases of falls. Vertebral anterior compression ranged from one-third to one-half, all classified as type A fractures. The mean preoperative Cobb angle was (23.3 ± 6.5)°. The study was approved by the institutional ethics committee.
Surgical Procedure
All surgeries were performed under general anesthesia in the prone position via a posterior midline approach. A longitudinal incision centered on the fractured vertebra was made, and paraspinal muscles were bluntly dissected to expose the facet joints.
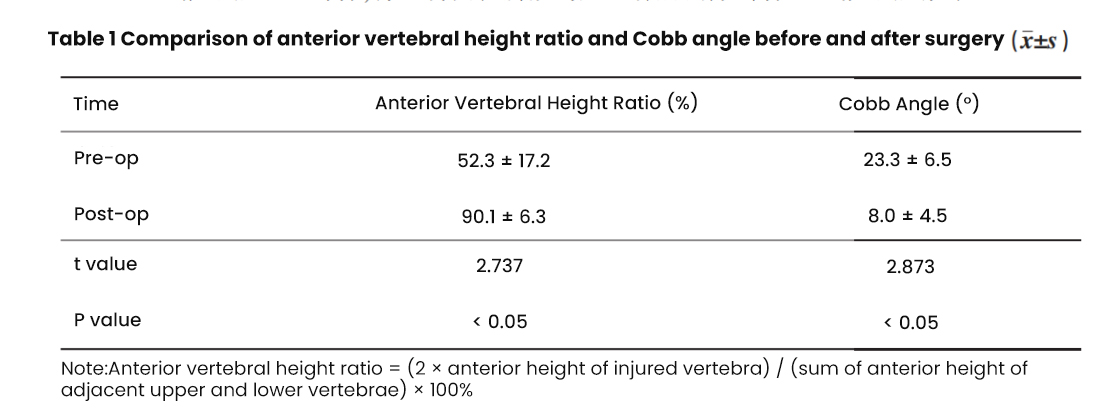
Pedicle screws were inserted into the pedicles of the injured vertebra (unilaterally) and bilaterally into adjacent vertebrae. After establishing the pedicle trajectory using an awl and probe, screws of appropriate length were inserted under C-arm fluoroscopic guidance. Rods were connected, and distraction reduction was achieved before final tightening.
For bone grafting, a puncture point slightly lateral to the screw entry site was selected. A working channel was established into the vertebral body via the pedicle. Under fluoroscopy, the cannula tip was positioned at the midline on the anteroposterior view and between the anterior one-third and one-half of the vertebral body on the lateral view.
Approximately 5–6 mL of self-setting calcium phosphate bone substitute (powder mixed with setting liquid) was injected. In bilateral screw placement cases, temporary removal of the rod on the grafting side was required before reinsertion and final fixation.
Representative Case
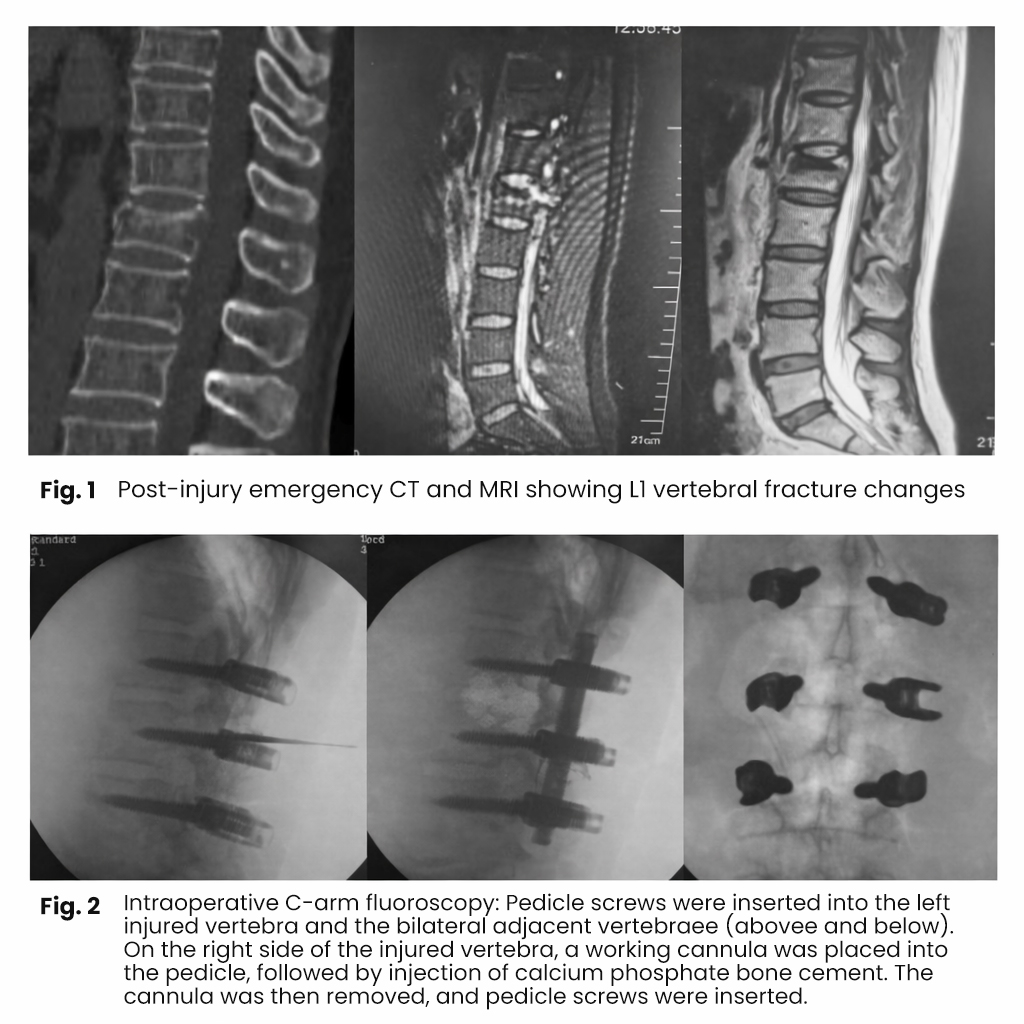
A 58-year-old female patient was admitted due to a fall injury. Clinical examination revealed tenderness and percussion pain in the thoracolumbar region, kyphotic deformity, and radiating pain in the right thigh. Lower limb muscle strength and sensory function were intact, and anal sphincter tone was normal.
Diagnosis: L1 vertebral compression fracture (TLICS score 5).
Treatment: Posterior pedicle screw-rod fixation combined with transpedicular grafting of self-setting calcium phosphate artificial bone.
Results
Follow-up duration ranged from 1.8 to 2.2 years (mean 1.9 ± 0.6 years). All surgical incisions healed primarily without complications such as neurological deficits.
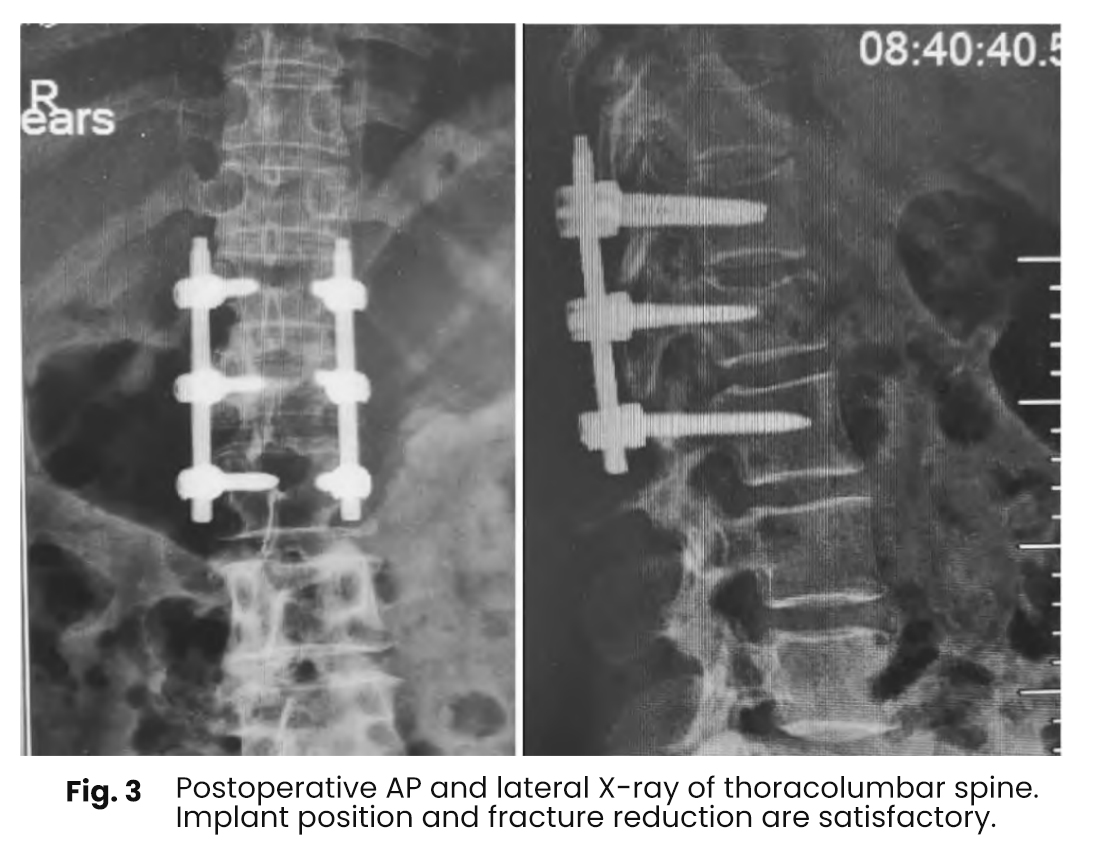
The anterior vertebral height recovered to (90.1% ± 6.3%) (t = 2.737, P < 0.05). Kyphotic Cobb angle correction ranged from 12° to 25°, with an average correction of 15.2° (t = 2.873, P < 0.05), indicating statistical significance.
Postoperative imaging demonstrated significant improvement in kyphosis compared to preoperative status. All cases showed satisfactory fixation and reduction, with no evidence of vertebral clefts or cystic degeneration within the vertebral body.

Discussion
Thoracolumbar vertebral fractures are common in orthopedic practice. Current consensus suggests:
TLICS score 4: conservative or posterior surgical treatment
TLICS score 5–6: posterior surgical treatment
TLICS score ≥7: anterior surgical treatment
However, delayed low back pain is more frequent in conservatively treated patients with a TLICS score of 4. Non-compliance with bed rest or early weight-bearing may lead to progressive vertebral collapse and kyphotic deformity, necessitating secondary surgery.
Surgical decision-making should consider vertebral compression severity and posterior ligamentous complex (PLC) integrity. When anterior compression exceeds 50% and/or PLC injury is suspected, surgical intervention is recommended. Preoperative imaging may not reliably detect PLC injuries, introducing uncertainty in treatment planning.
From an enhanced recovery perspective, surgical treatment yields better outcomes in patients with significant compression or suspected PLC injury. Although satisfactory reduction can often be achieved with screw-rod systems, postoperative loss of vertebral height and Cobb angle may still occur, particularly after implant removal.
Radiographically restored vertebral height may represent a “shell-like” appearance, while internal fracture healing remains incomplete. In this study, transpedicular injection of self-setting calcium phosphate was used to fill the vertebral body, promoting internal healing.
This technique is simple, avoids donor site morbidity associated with autologous bone grafting, and enhances fracture healing. Bone grafting does not provide immediate mechanical support; therefore, robust internal fixation remains essential to prevent early failure.
The primary role of bone grafting is to fill intravertebral voids, prevent cystic degeneration and residual clefts, and facilitate biological healing. This ultimately restores vertebral height, enhances spinal stability, and reduces complications such as screw loosening, breakage, and recurrent compression.
The maintenance of vertebral height and Cobb angle depends primarily on fixation strength, while transpedicular bone grafting promotes fracture healing. Short-segment pedicle screw fixation combined with self-setting calcium phosphate grafting effectively reduces postoperative pain, prevents vertebral cavity formation, and achieves satisfactory clinical outcomes.
Compared with autologous iliac bone grafting, this method is safer, simpler, and avoids donor site complications, while providing effective osteoconductive properties and promoting bone defect repair.